
What is AOMSI?
- claytonchiropractic
- 2 hours ago
- 8 min read

Welcome to the second podcast. Today’s podcast will fit in well with the first podcast which was all about ligaments. The first podcast talked about the makeup of ligaments, how they get injured, what the inadequate healing process for damaged ligament is like and how to manage ligament damage.
Today’s podcast will discuss alteration of motion segment integrity or AOMSI. The term AOMSI is used frequently in the person injury world. Today I want to talk about the origins of AOMSI. Before we get into today’s article I want to explain what AOMSI is for those who do not know. AOMSI is ligament damage. Ligament damage that has altered the integrity of a motion segment or a joint. Sometimes the term ligament laxity has been used in place of AOMSI, but as you will see in today’s article AOMSI is more than a lax ligament it is typically torn ligaments.
Today’s article is Biomechanical analysis of Clinical Stability in the Cervical Spine. This article was written by White et al. and published in the Clinical Orthopedics and Related Research journal June of 1975. This article was written by a group of orthopedic surgeons and Panjabi who is the leading expert on biomechanics of the spine.
It is important to understand why a group of surgeons wrote this article. In the first paragraph they given a hint as to why this article was written, by saying what constitutes an unstable spine is not always clear and indications to treat an unstable spine are not well defined. To me it is clear that this group of surgeons was looking for clinical indications of when to fuse cervical spines and justification for insurance companies to pay for these fusions.
They set up a study that looked at motion segments of the cervical spine below C2. Motion segments consist of a top vertebra the disc and a bottom vertebra. These motion segments had loads applied to them that simulate flexion and extension loads. This experiment used 8 fresh cadavers with specimens frozen in a bag to preserve moisture. All testing was done in high humidity chamber using cold stream vaporizer to preserve the natural hydration of bones and ligaments.
Care was taken to leave the vertebra and ligaments unencumbered. Simulating flexion and extension loads these motion segments were pulled apart to assess for failure in horizontal translation and rotation.
One thing that surprised the authors of the study was Quote “failure commonly occurred with sudden, complete separation of the upper vertebra form the lower vertebra”. And “ it was generally found that the majority of the ligaments had to be transected before failure occurred” UNQUOTE. This study showed similar results to the article from the first podcast showing that ligaments when damaged will undergo micro tearing and then complete tearing. Today’s study showed quote “ligaments would often result in complete, instantaneous failure” Unquote.
They were able to show that this sudden and complete instantaneous failure of the ligaments can be seen with translation or when the top vertebra moved horizontal to the bottom one by 2.67mm. This sudden and complete instantaneous failure of ligaments can also be seen with change in angular displacement Or when the top vertebra is pulled so hard the angle increased to 10.7 degrees. For those familiar with AOMSI this should sound close to the 3.5mm translation or 11 degrees change in angular motion.
The authors needed a way to assess this type of damage on living patients and relied on flexion and extension x-rays of the cervical spine. Flexion and extension x-rays are done with a lateral or side view of the cervical spine. When a side view x-ray is taken the neck is not right up against the x-ray panel since the shoulder would be up against the panel creating a gap. This gap creates a magnification of the spine. This is similar to holding your hand up to a flashing and creating a large shadow of the wall. This magnification of the cervical spine would make the 2.67mm translation calculation off on x-rays. To adjust for this magnification the authors calculated that 3.5mm translation on x-rays would be the same as the 2.67mm translation seen on the cadaver studies. This is where the 3.5mm translation for AOMSI came from.
What is angular displacement? On a side view x-ray if we draw a line on the bottom of the vertebra we can measure angles of the different motion segments. This study showed that once motion segments exceed 10.7 degrees displacement we have torn the majority of ligaments and have complete and sudden failure. The study uses the adjacent motion segments to assess for more than 10.7 degrees change. For simplicity the study moved from 10.7 degrees change in angular motion to 11 degrees. This is not due to x-ray magnification since this would not change angles.
There are lots of ligaments in the cervical spine the 2 large ones go from the front and the back of the vertebral bodies. The front ligament is called the anterior longitudinal ligament Or ALL and the back one is called the posterior longitudinal ligament or PLL. When the spine shows instability on extension x-rays this study showed that the ALL was the more damaged ligament. This study showed that the PLL is the more damaged ligament on flexion.
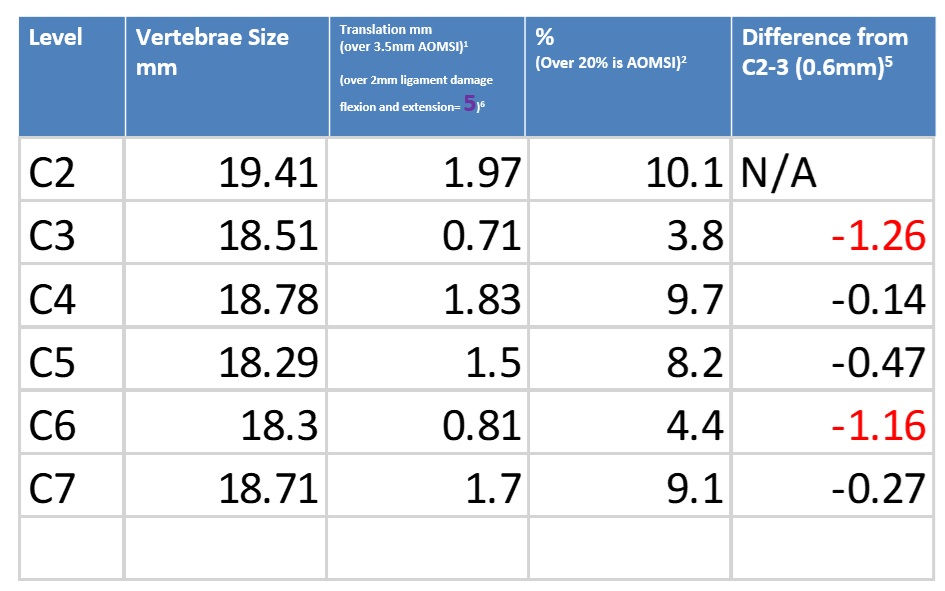
There are dozens of computer software programs out there to help with AOMSI measurements. I have seen a lot of different programs and they all seem to measure differently. This is a simple process and I believe no program is necessary to do this for providers. The study showed that for horizontal displacement 2 discrete points on the inferior posterior endplate are marked. Then perpendicular lines are drawn and the distance between these lines is measured. If it is at 3.5mm or greater then AOMSI is present. Most x-rays now days are digital and measuring mm on digital x-rays is very simple.
Measuring change in angular motion is equally simple. Starting at C2 lines are drawn on bottom of the vertebral body. Angles are measured between each motion segment and the motion segment above and below. If there is 11 degrees more or less at a single motion segment than the level above and below then AOMSI is present. This is simple to do on digital x-rays.
AOMSI in the American Medical Association’s Guides to the Evaluation of Permanent Impairment has led to a lot of confusion. The 5th edition first came out in the year 2000. There was an error in printing for the AOMSI section. An Errata was published in March of 2002 that corrected this error. I feel like this initial error led to many different ways of measuring AOMSI for an impairment rating. The original 5th edition allowed for change in angular motion from flexion and extension views, but the Errata only allows for change in angular motion from the flexion view. The original 5th edition made the mistake of subtracting the flexion angle from the extension angle and coming up with a new measurement. This was corrected in the Errata and restored to the guidelines from the study we have gone over today where it compares each angle to the level above and below. This is probably one of the biggest things I seen software companies doing. The 5th edition originally reported horizontal translation as 3.5mm as seen in the study we went over and has not changed with the Errata. Given the fact that the study showed complete and sudden failure of ligaments once the threshold was crossed the AMA 5th edition allows for a 25% whole body impairment rating.
The AMA 6th edition came out in 2008 and was updated 7/1/2021. The concepts for AOMSI have changed with the 6th edition in a few unique ways. Translation is measured the same, but for an impairment of AOMSI instead of 3.5mm translation we now need 20% translation of the vertebra. I have no idea why they changed from 3.5mm to 20% translation, but this is a similar number on most studies I have seen. The 6th edition measures change in angular motion the same as the 5th edition besides they now require a change of 11 degrees from both the upper and lower cervical vertebra. The 6th edition has categorized AOMSI in the motion segment lesions category with disc herniations. To move up to up beyond a class 1 impairment rating the patient needs to have radiculopathy (nerve root compression). Radiculopathy is often seen with disc herniations, but not AOMSI. I disagree with the AMA guides on requiring radiculopathy for a higher impairment rating with AOMSI. Without radiculopathy an AOMSI diagnosis in the 6th edition will be from 4-8% whole body impairment rating.
I have seen different software do the measurements all different ways, but have yet to see one that does it according to the White study we went over today or the AMA ways. Fortunately, no software is needed to measure angles and mm. I have seen a couple software programs that have decided they do not like the all or nothing impairment rating seen with AOMSI and have decided to pro rate impairment ratings. On the surface this sounds like a good idea. Why would 11 degrees be AOMSI with a large impairment rating and 10 degrees be no AOMSI with a small impairment rating for strain/sprain?
This feeling of unfairness has led software programs to give prorated impairment ratings. Although this sounds right, we need to remember the study we went over today and last time. Ligaments will undergo minor tearing or sudden and complete failure. The sudden and complete failure can be shown at 11 degrees change in angular motion and 3.5mm translation. If we are below these levels we are likely dealing only with minor tearing of ligaments. Although all ligament damage can be significant minor vs. complete tearing is a dramatic difference.
Real world
I had a patient that was in a drive through restaurant. A drunk driver in a large SUV pulled in really fast and collided with the rear of her vehicle. She was in a lot of pain and flexion and extension x-rays were ordered. The motion x-rays showed she has 11.16 degrees change in angular motion at C3-4 compared with C2-3 and 13.1 degrees change from C4-5. This shows that she has AOMSI in her cervical spine. I was able to use today’s article the Biomechanical analysis of Clinical stability in the cervical spine to help with her final report. With this study I was able to show that she has AOMSI which is catastrophic or complete ligament damage at her C3-4 level. This is not a simple strain/sprain injury. As seen in last weeks podcast this type of injury will lead to osteoarthritis and this would be visible on x-rays. Given the lack of osteoarthritis it was clear that this AOMSI was much more likely than not directly related to the MVC and not pre-existing.
This complete ligament damage in her cervical spine is very significant. I covered this briefly on the last podcast, but the persistent permanent complications from this type of ligament damage are very significant. This patient will need ongoing management of her injuries. The study we went over today came out in 1975 and was used to clinically justify cervical fusions. Is this still the case? We no longer fuse the spine with just clinical instability. The cervical spine fusion now days are typically done when there is significant nerve or spinal cord compression. Her spine will deteriorate over time and develop arthritis. Her report showed that over time she may develop nerve or spinal cord compression and then need a surgical consultation directly related to the MVC. The neurosurgeon I worked with agreed in his report that she may need surgical fusion 15-20 in the future related to her MVC.


Comments